A 26-year-old man presents to ED with dull, pleuritic chest pain after being hit in the chest by a soccer ball during a match. The pain radiates to the back and is exacerbated by coughing. Shortness of breath is noted. On examination, the patient has a high-pitched voice and crepitus over the neck and clavicles. Chest expansion is symmetrical and the lungs are clear bilaterally. There is no hyper-resonance on percussion. A crunching sound during systole is auscultated over the precordium. The ECG is normal. A chest radiograph is ordered (see picture).
What is the most likely diagnosis?
Correct!
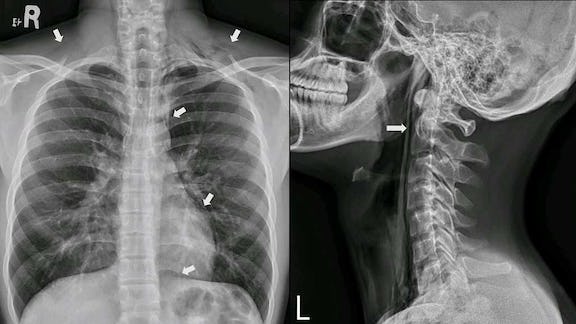
This is a case of pneumomediastinum due to a traumatic force on the chest wall. The X-ray shows radiolucent streaks of air along the left heart border, extending towards the aortic arch and the trachea-bronchial tree (see above image).
Radiolucency is seen between the diaphragm and the lower heart border, and in the bilateral supraclavicular fossa. No obvious visceral pleural line indicative of pneumothorax is noted. A lateral chest radiograph reveals air in the retropharyngeal space (see image). CT imaging confirms pneumomediastinum without airway or oesophageal injury.
The patient is admitted for oxygen therapy after three hours of observation. A repeat chest radiograph taken after four days shows regression of pneumomediastinum and the patient is discharged.
Pneumomediastinum is characterised by the presence of air in the mediastinum, occurring spontaneously or secondary to traumatic lung injury. Patients usually present with pleuritic chest pain and shortness of breath, similar to pneumothorax and pneumopericardium. Distinctive features of pneumomediastinum include high-pitched voice (also termed rhinolalia), subcutaneous emphysema and Hamman’s crunch during auscultation.
Diagnosis can be made based on radiolucency outlining mediastinal structures on plain radiograph. CT scans are usually performed to confirm pneumomediastinum or to rule out other potentially life-threatening aerodigestive injuries.