
Leukemia is a type of cancer that affects the blood and bone marrow. It is characterized by the uncontrolled proliferation of abnormal white blood cells. There are several types of leukemia, each with distinct features, but generally, they can be categorized into acute and chronic forms. Here’s a detailed discussion:
Causes
- Genetic Factors: Certain genetic mutations and chromosomal abnormalities can contribute to the development of leukemia.
- Environmental Factors: Exposure to high levels of radiation, certain chemicals like benzene, and chemotherapy drugs can increase the risk.
- Viral Infections: Some viruses, such as the Human T-lymphotropic virus, have been linked to certain types of leukemia.
- Immune System Disorders: Previous immune system disorders or treatments may increase risk.
- Family History: A family history of leukemia increases the risk, although familial leukemia is rare.
Diagnosis
- History:
- Symptoms: Fatigue, fever, frequent infections, easy bruising or bleeding, weight loss, bone or joint pain, swollen lymph nodes, and abdominal discomfort (due to an enlarged spleen or liver).
- Previous Medical Treatments: History of chemotherapy or radiation therapy for other cancers.
- Exposure History: Prior exposure to radiation or chemicals.
- Examination:
- Palpation for enlarged lymph nodes,
- Abdominal examination for liver, or spleen.
- Checking for signs of anemia (pallor),
- Checking for signs of thrombocytopaenia ie petechiae, or bruising.
- Investigations:
- Blood Tests: FBC often shows abnormal white blood cell counts. Peripheral blood smear to look at the morphology of blood cells.
- Bone Marrow Aspiration and Biopsy: To examine bone marrow cells under a microscope and check for leukemia cells.
- Cytogenetic Analysis: To detect chromosomal abnormalities in leukemia cells.
- Immunophenotyping: To determine the type of leukemia.
Differential Diagnosis (DDx)
- Aplastic Anemia: Characterized by pancytopenia and hypocellular bone marrow.
- Infectious Mononucleosis: Caused by the Epstein-Barr virus, can mimic leukemia symptoms.
- Other Hematologic Cancers: Like lymphoma or myelodysplastic syndromes.
- Bone Marrow Failure Syndromes: Such as myelofibrosis.
- Inflammatory or Infectious Conditions: That cause leukocytosis.
Management
- Chemotherapy:
- The mainstay of treatment for most types of leukemia. It can be intensive, especially for acute leukemias.
- Targeted Therapy:
- Uses drugs that target specific vulnerabilities in leukemia cells. For example, tyrosine kinase inhibitors in chronic myeloid leukemia (CML).
- Radiation Therapy:
- Sometimes used to control bone pain or to shrink an enlarged spleen or lymph nodes.
- Bone Marrow/Stem Cell Transplant:
- In some cases, especially if chemotherapy is not effective.
- Supportive Care:
- Blood transfusions, antibiotics for infections, and medications to manage symptoms like nausea.
- Follow-Up and Monitoring:
- Regular follow-ups to monitor blood counts and assess for disease progression or remission.
- Counseling and Support:
- Psychological support for patients and families to cope with the diagnosis and treatment.
Conclusion
Leukemia treatment and prognosis vary widely depending on the type of leukemia, the patient’s age, and other health factors. Advances in treatment, including targeted therapies and stem cell transplantation, have significantly improved outcomes for many patients with leukemia. Early detection and a multidisciplinary approach to care are critical for optimal outcomes.
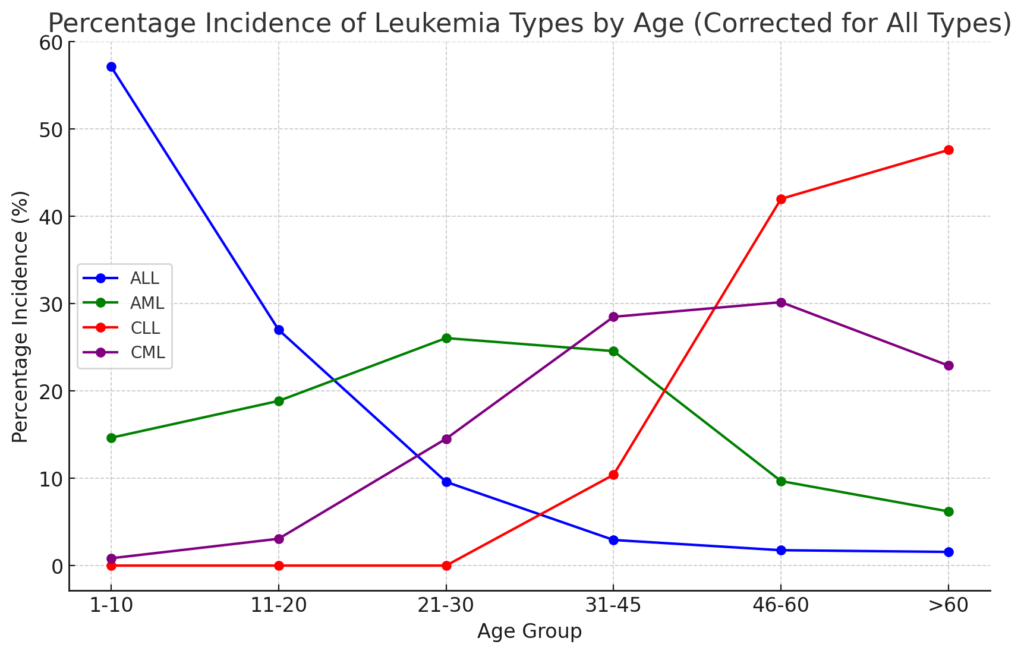
Acute Lymphoblastic Leukemia (ALL)
- Epidemiology: Most common in children, but also occurs in adults.
- Pathophysiology: Characterized by the overproduction of immature lymphocytes (lymphoblasts).
- Symptoms: Fatigue, fever, bleeding or bruising, bone pain, lymphadenopathy, hepatosplenomegaly.
- Diagnosis: Complete blood count, bone marrow biopsy, immunophenotyping.
- Treatment: Intensive chemotherapy, targeted therapy (e.g., tyrosine kinase inhibitors for BCR-ABL-positive ALL), and possibly stem cell transplantation. Prognosis varies, generally better in children.
Acute Myeloid Leukemia (AML)
- Epidemiology: Any age, more common in adults
- Pathophysiology: Rapid growth of abnormal myeloid cells.
- Symptoms: Similar to ALL, with more pronounced myelosuppression leading to anemia, thrombocytopenia, and neutropenia.
- Diagnosis: CBC with differential, bone marrow biopsy, cytogenetic analysis.
- Treatment: Chemotherapy (induction and consolidation phases), targeted therapies (e.g., FLT3 inhibitors), and stem cell transplantation in selected cases. The prognosis is variable and often poorer in older adults.
Chronic Lymphocytic Leukemia (CLL)
- Epidemiology: Most common form of leukemia in adults in Western countries.
- Pathophysiology: Accumulation of functionally incompetent lymphocytes.
- Symptoms: Often asymptomatic initially; may present with lymphadenopathy, fatigue, anemia, and infection susceptibility.
- Diagnosis: Often incidental finding on CBC, flow cytometry for immunophenotyping, bone marrow biopsy.
- Treatment: Observation in early stages; chemotherapy, monoclonal antibodies (e.g., rituximab), targeted agents (e.g., ibrutinib) in symptomatic disease. Generally, it has an indolent course but can transform into a more aggressive disease.
Chronic Myeloid Leukemia (CML)
- Epidemiology: Affects adults, rarely in children.
- Pathophysiology: Characterized by the presence of the Philadelphia chromosome, which results in the BCR-ABL fusion gene.
- Symptoms: Fatigue, weight loss, splenomegaly, fullness in the abdomen, easy bleeding.
- Diagnosis: CBC showing elevated white blood cells, bone marrow biopsy, cytogenetic analysis to identify the Philadelphia chromosome.
- Treatment: Tyrosine kinase inhibitors (e.g., imatinib) are the mainstay of treatment, offering good long-term prognosis. Allogeneic stem cell transplantation may be considered in resistant cases.
Conclusion
While ALL, AML, CLL, and CML share the common feature of being leukemias, their presentation, progression, and treatment strategies vary significantly. Advances in the understanding of their molecular biology have led to more targeted therapies, significantly improving outcomes, particularly in CML and certain subtypes of ALL and AML. Early diagnosis and tailored treatment are crucial in the management of these conditions.