
Tim is a 45-year-old who presents with left cheek swelling and bruising following a physical altercation the day before.
Tim took a few solid punches to the left cheek and eye, which have become progressively painful, bruised and swollen.
He attended an after-hours clinic in the early hours of the morning and was referred for an X-ray of the facial bones and follow-up the next day.
On examination, there is significant left periorbital bruising and swelling.
Pupils are equal and responsive to light and accommodation, and extraocular movements are normal, with no diplopia.
Facial sensation is intact. He has localised left infraorbital rim tenderness, with palpable crepitus.
What is the diagnosis?
Correct!
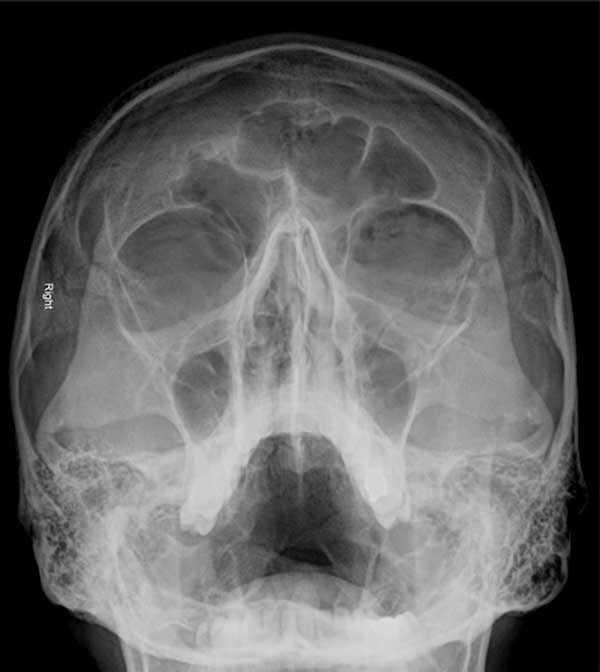
The occipitomental (Waters’ view) X-ray shows the presence of a left black eyebrow sign: a crescent-shaped radiolucency resembling an eyebrow.
This is typically the result of an orbital wall or blowout fracture. The fracture causes air to leak from the maxillary or ethmoidal sinus into the superior aspect of the orbit, giving the appearance of an eyebrow on the occipitomental view (angled posterior–anterior skull X-ray with patient positioned gazing slightly upward).
Orbital blowout fractures occur when there is a fracture of one of the walls of orbit but the orbital rim remains intact.
The usual mechanism is a direct blow to the central orbit from a fist or ball. Inferior blowout fractures are the most common form.
The risk posed by this injury is that it causes orbital fat to prolapse into the maxillary sinus, which may cause associated prolapse of the inferior rectus muscle.
This will result in limited upward gaze on the affected side and associated diplopia.
Enophthalmos may occur if the globe displaces posteriorly as a result of prolapsed tissue in the maxillary sinus.
Associated injury to the infraorbital nerve may occur, resulting in decreased sensation along the cheek, upper lip or upper gingiva.
Serious life- or sight-threatening injuries must first be assessed and managed in the setting of suspected orbital fractures.
CT is the imaging modality of choice for the facial bones and is recommended in the setting of periorbital trauma if there is clinical evidence of a fracture, reduced extraocular movement, reduced visual acuity, severe pain or limited examination (due to swelling or altered mental state of the patient).
An occult maxilla fracture may be indicated by an air-fluid level in the maxillary sinus rather than the black eyebrow sign. A zygomaticomaxillary complex fracture is characterised by the disruption of the lateral orbital wall, orbital floor, zygomatic arch and maxillary sinus.
Tim is referred to ED, and a facial CT confirms an inferior orbital wall fracture. He is reviewed the same day in ED by the local hospital maxillofacial surgeon.