
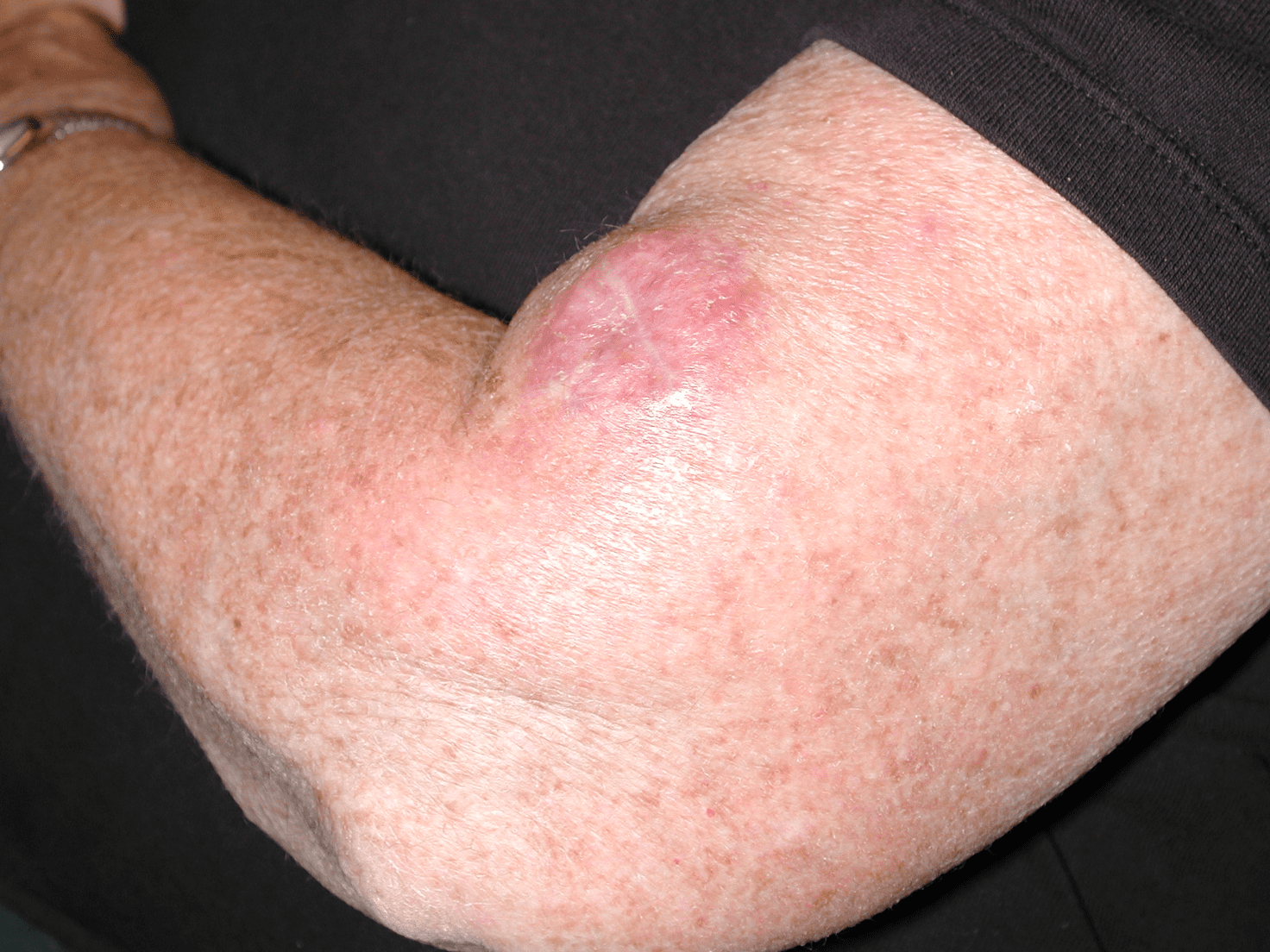
A 71-year-old retired firefighter presents with a solitary nodule on his left arm. The patient reports that the lesion has grown rapidly over a four-week period. He denies any bleeding or tenderness.
His past medical history includes multiple non-melanoma skin cancers; recurrence of multiple myeloma, for which he previously received daratumumab; and prostate cancer, which has been resected. He also has a family history of melanoma (maternal).
On examination, there is a non-tender solitary erythematous nodule on his left proximal arm. He has no cervical oraxillary lymphadenopathy.
What is the most likely diagnosis?
Correct!
Merkel cell carcinoma is a rare neuroendocrine skin tumour. These carcinomas can metastasise locally or to distant sites. They typically affect elderly Caucasian males and occur on sun-exposed regions.
The clinical presentation of Merkel cell carcinoma is often a rapidly expanding firm erythematous nodule on sun-exposed areas of skin, such as head and neck regions.
Merkel cell polyomavirus infection is involved in the aetiology of the condition. Merkel cell polyomavirus can integrate its DNA into the genome of an immunocompromised host, mediating carcinogenesis.
Merkel cell carcinoma can enhance expression of programmed cell death ligand-1 that consequently inhibits T-cell expansion and stimulates exhaustion of T-cells. This stimulates localised immune suppression and tumour immune evasion.
Risk factors for Merkel cell carcinoma include older age, immunosuppression and UV exposure. A skin biopsy and evaluation of the sentinel lymph nodes are required for diagnosis.
Differential diagnosis includes basal cell carcinoma, squamous cell carcinoma, amelanotic melanoma, pyogenic granuloma, keratoacanthoma and epidermal inclusion cyst.2 Unlike Merkel cell carcinoma, basal cell carcinomas are usually slow growing, smooth and red.
Squamous cell carcinoma is typically keratotic and rapidly growing. Amelanotic melanoma consists of lesions that are poorly pigmented or non-pigmented and is inversely related to a family history of melanoma.
For local Merkel cell carcinoma lesions, treatment involves local excision. Adjuvant radiotherapy may also be performed locally in low-risk patients. For patients with Merkel cell carcinoma that has spread to the regional lymph nodes, lymph node dissection is recommended together with radiotherapy.
For metastatic disease, a combination of treatment options may be considered, such as radiation therapy, immunotherapy, chemotherapy and surgery.
In this case, a skin biopsy confirmed localised Merkel cell carcinoma. The patient underwent wide local excision surgery and radiotherapy.