
Damian is a 64-year-old retired labourer. He has a history of spinal stenosis, chronic pain and traumatic brain injury. His medications include duloxetine and tapentadol.
Damian presents with a six-month history of right nipple change. It is darker, mildly itchy and feels much thicker than the left. There is no nipple discharge. He has no pain but is concerned about what is causing the change.
He has had significant sun exposure in the past, with no significant family history of cancer.
Clinically both breasts and axillae are normal on palpation except for the areola region of his right breast (pictured, post-punch biopsy) which is thickened and hyperpigmented.
Damian declines any breast imaging. Given this a punch biopsy is performed.
What is the most likely diagnosis?
Correct!
The clinical findings are consistent with naevoid hyperkeratosis of the nipple.
This condition presents as a verrucous appearing pigmented area of thickening, typically confined to the nipple and areola.
The plaques are usually asymptomatic, though may cause itch. The cause is unclear.
These lesions do not require treatment, apart from for cosmesis, in which case cryotherapy or keratolytics may be of benefit, although carry a risk of hypopigmentation. Topical steroids may be trialled for itch.
Diseases of the male nipple-areola-complex are relatively uncommon. Some of the potential causes are associated with significant morbidity and mortality.
The key differential diagnosis of concern in this case was Paget’s disease of the nipple, as this malignant condition carries significant morbidity and mortality. Paget’s disease is uncommon, and especially rare in males.
The fact that there was no palpable mass on breast examination was reassuring, but not decisive for the diagnosis. However, the suggestion of any breast imaging was unacceptable to the patient, notwithstanding the risk of missing breast malignancy.
The diagnosis of seborrhoeic keratosis was also considered, but the uniformity and confinement to the nipple area made this less likely.
The possibility of a melanoma was also entertained but this condition is also exceedingly uncommon.
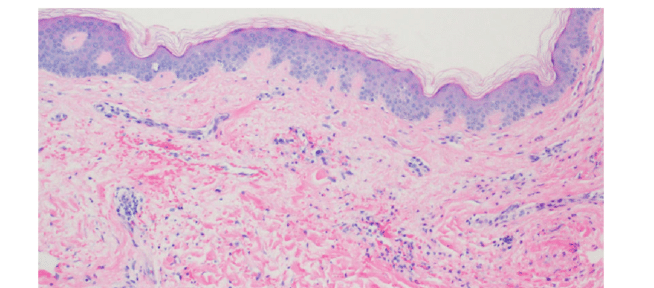
In this case punch biopsy of the areola revealed orthokeratotic hyperkeratosis, papillomatosis, keratotic plugging and a mild dermal perivascular lymphocytic infiltrate, consistent with naevoid hyperplasia of the nipple.