Developmental dysplasia of the hip (DDH) is a condition where there is a structural abnormality in the hips caused by abnormal development of the fetal bones during pregnancy. This leads to instability in the hips and a tendency or potential for subluxation or dislocation. These structural abnormalities have the potential to persist into adulthood leading to weakness, recurrent subluxation or dislocation, an abnormal gait and early degenerative changes.
DDH is either picked up during the newborn examinations or later when the child presents with hip asymmetry, reduced range of movement in the hip or a limp.
Risk Factors
- First degree family history
- Breech presentation
- Multiple pregnancy
Screening
DDH is screened for on the neonatal examination at birth and 6-8 week old. When examining, look for symmetry in thehips, leg length, skin folds and hip movements. Findings that may suggest DDH are:
- Different leg lengths
- Restricted hip abduction on one side
- Significant bilateral restriction in abduction
- Difference in the knee level when the hips are flexed
- Clunking of the hips on special tests
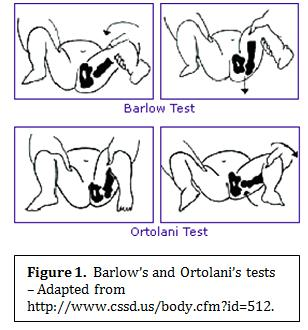
There are two special tests used to check for DDH:
- Ortolani test
- Barlow test
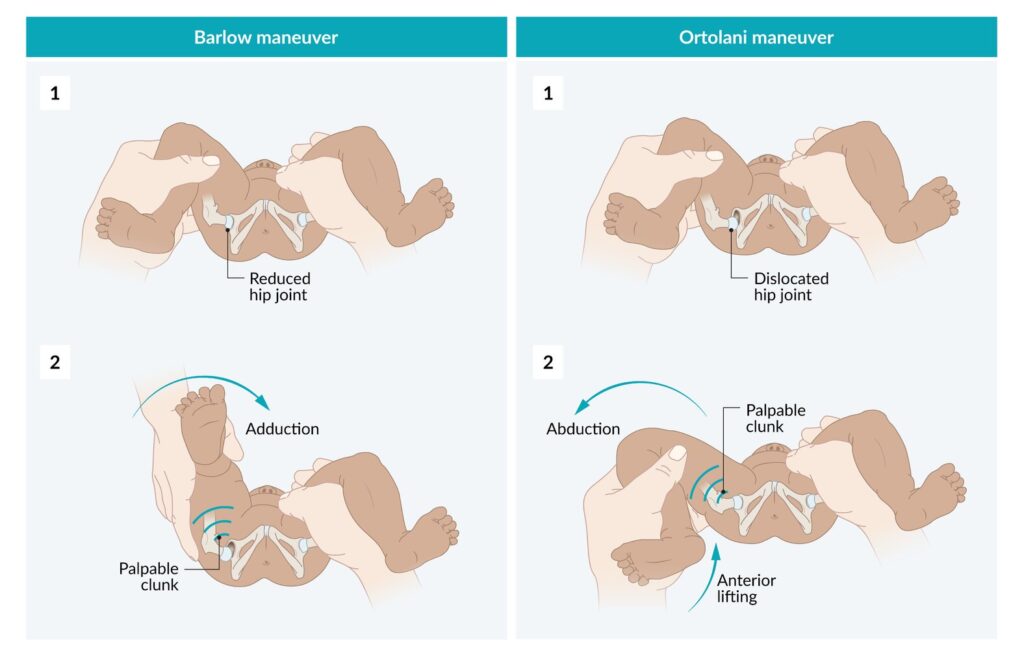
Ortolani test is done with the baby on their back with the hips and knees flexed. Palms are placed on the baby’s knees with thumbs on the inner thigh and four fingers on the outer thigh. Gentle pressure is used to abduct the hips and apply pressure behind the legs with the fingers to see if the hips will dislocate anteriorly.
Barlow test is done with the baby on their back with the hips adducted and flexed at 90 degrees and knees bent at 90 degrees. Gentle downward pressure is placed on knees through femur to see if the femoral head will dislocate posteriorly.
BP OA – Barlow Posterior, Ortolani Anterior
Clicking is a common examination finding and is usually due to soft tissue moving over bone. When this is the cause an ultrasound will be normal. Isolated clicking without any other features does not usually require an ultrasound unless there are other concerns. Clunking is more likely to indicate DDH and requires an ultrasound.
Diagnosis
Where children are suspected of having DDH, ultrasound of the hips is the investigation of choice and can establish the diagnosis. All children with risk factors or examination findings suggestive of DDH should have an ultrasound.
Xrays can also be helpful, particularly in older infants.
Management
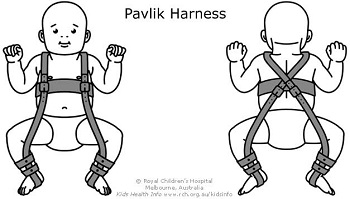
Treatment typically involves a Pavlik harness if the baby presents at less than 6 months of age. The Pavlik harness is fitted and kept on permanently, adjusting for the growth of the baby. The aim is to hold the femoral head in the correct position to allow the hip socket (acetabulum) to develop a normal shape. This harness keeps the baby’s hips flexed and abducted (frog position) The child is regularly reviewed and the harness is removed when their hips are more stable, usually after 6 – 8 weeks.
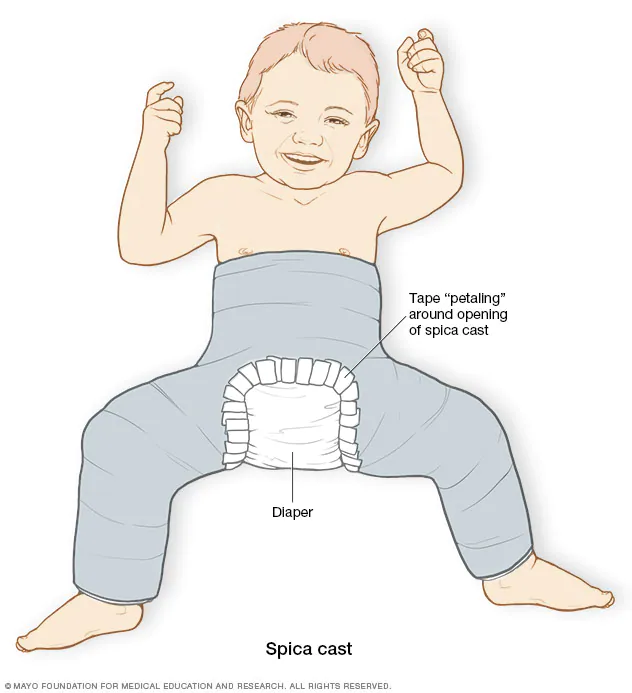
Surgery is required when the harness fails or the diagnosis is made after 6 months of age. After surgery is performed, an hip spica cast is used to immobilises the hip for a prolonged period.